Washington Severe Mental Illness Information, Laws, & Helpful Resources
The term severe mental illness (SMI) includes schizophrenia spectrum disorders, severe bipolar disorder, and major depression with psychotic features. These disorders put an individual at high risk for criminalization and preventable tragedies such as victimization and suicide. Every state has different laws and policies around accessing treatment for SMI and some states have more resources and treatment options than others. Here you will find state-specific resources for navigating the SMI treatment system, an evaluation of local laws, as well as state SMI data and research.
Family Resources in Resources in Washington
- Washington State Health Care Authority Mental Health Services (hca.wa.gov) Resources and contacts
- Washington Recovery Help Line – 1-866-789-1511 (warecoveryhelpline.org) Resources for mental illness and addiction
- Behavioral Health Agencies Directory (doh.wa.gov) Provider list by county
- New Journeys early intervention (newjourneyswashington.org) First episode psychosis program with family resources and an online referral form
- University of Washington Spirit Lab (uwspiritlab.org) Cognitive behavioral therapy for psychosis (CBTp) training and resources for family caregivers
- Office of Behavioral Health Advocacy (obhadvocacy.org) Support for disputes and provider searches
- Office of Forensic Mental Health Services (dshs.wa.gov) Mental health services in the criminal legal system
- Forensic Navigator Program (dshs.wa.gov) Community-based competency restoration services for eligible people charged with a crime and found unable to act in their own defense
- NAMI Washington (namiwa.org) Support groups, training, information
- Disability Rights Washington (disabilityrightswa.org) Protection and advocacy for individuals with disabilities
- Homeless Information: Washington |U.S. Department of Housing and Urban Development (hud.gov/states/washington) Shelter locator and links to local resources
- Department of Corrections Inmate Search (doc.wa.gov) Search for someone in prison by name and DOC number
- Washington State Bar Association (wsba.org) Legal assistance
How many people in Washington have SMI?
individuals with severe mental illness.
individuals with SMI who receive treatment in a given year.
of the adult population is estimated living with a SMI in the United States.
State psychiatric hospital beds in Washington
2023 total beds: 1,034
- Civil beds: 431
- Forensic beds: 603
2023 beds per 100,000 people: 13.3
Click here for more information about state psychiatric hospital beds in Washington.
A minimum of 50 beds per 100,000 people is considered necessary to provide minimally adequate treatment for individuals with severe mental illness. Washington fails to meet this minimum standard.
For Additional Information
Data is a powerful tool to advocate for change. Curious about a specific data point in your state? Reach out to us at ORPA@treatmentadvocacycenter.org
Fast Facts on SMI in Washington
Deinstitutionalization, outdated treatment laws, discriminatory Medicaid funding practices, and the prolonged failure by states to fund their mental health systems drive those in need of care into the criminal justice and corrections systems.
15%
2,190
1,034
2 to 1
2021 Washington State Mental Health Agency's expenditures
Every state receives block grant funding from the federal government to provide mental health services to their community. Below is some information about how these dollars are spent and compares to other state spending.
$1,747,629,380
34%
$6,376
2.9%
Washington's Treatment Laws
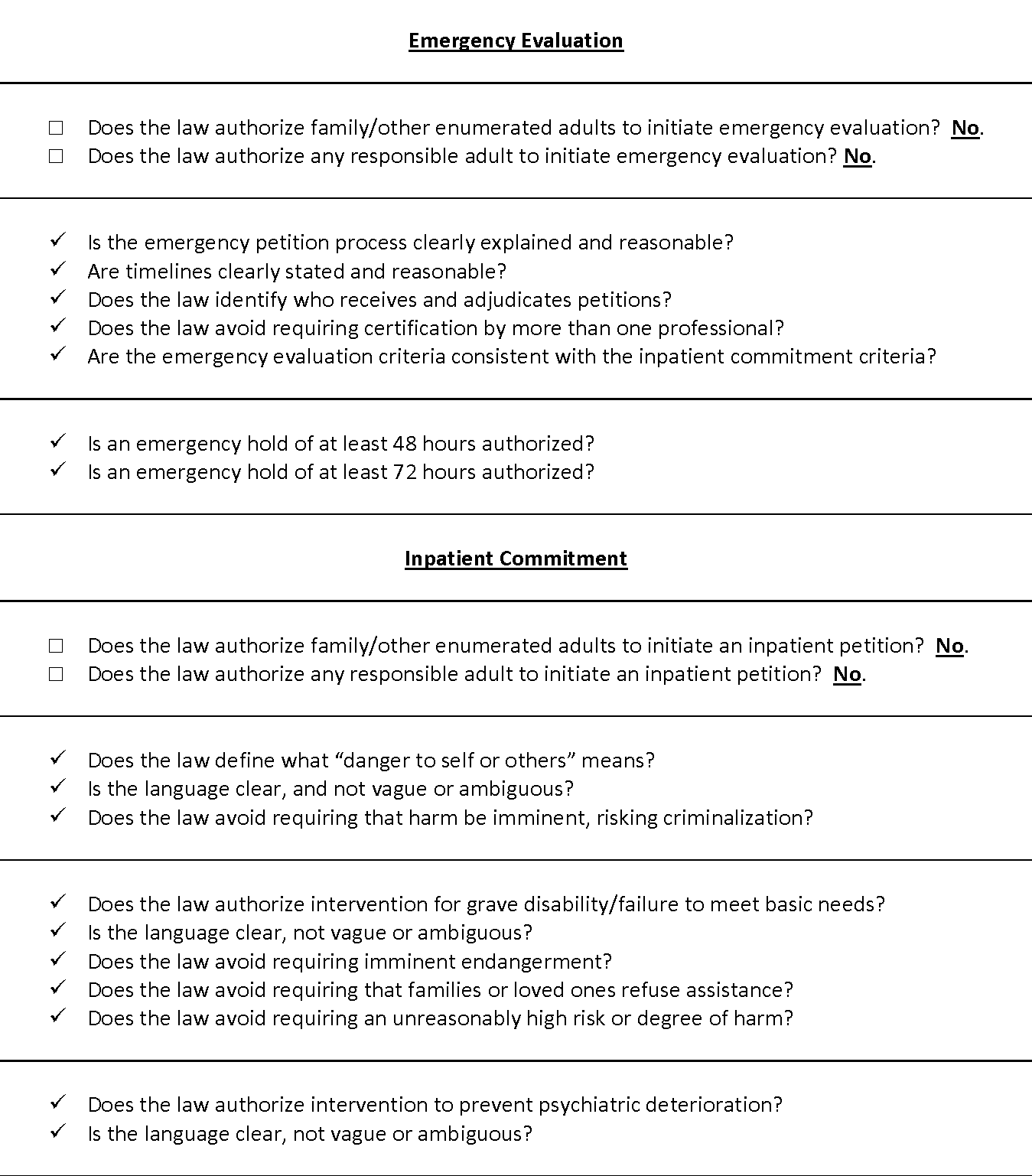
REV. CODE WASH. § 71.05.150(1). When a designated crisis responder receives information alleging that a person, as a result of a mental disorder [meets the criteria for inpatient commitment], the designated crisis responder may, after investigation and evaluation of the specific facts alleged and of the reliability and credibility of any person providing information to initiate detention or involuntary outpatient treatment, if satisfied that the allegations are true and that the person will not voluntarily seek appropriate treatment, file a petition for initial detention under this section or a petition for involuntary outpatient behavioral health treatment [.] Before filing the petition, the designated crisis responder must personally interview the person, unless the person refuses an interview, and determine whether the person will voluntarily receive appropriate evaluation and treatment at an evaluation and treatment facility, crisis stabilization unit, triage facility, or approved substance use disorder treatment program. REV. CODE WASH. § 71.05.150(2)(a) A written order of apprehension to detain a person with a behavioral health disorder to a designated evaluation and treatment facility, a secure withdrawal management and stabilization facility, or an approved substance use disorder treatment program, for a period of not more than one hundred twenty hours for evaluation and treatment, may be issued by a judge of the superior court upon request of a designated crisis responder (…) whenever it appears to the satisfaction of a judge of the superior court: (i) That there is probable cause to support the petition; and (ii) That the person has refused or failed to accept appropriate evaluation and treatment voluntarily. REV. CODE WASH. § 71.05.153(1). When a designated crisis responder receives information alleging that a person [meets the criteria for emergency evaluation], after investigation and evaluation of the specific facts alleged and of the reliability and credibility of the person or persons providing the information if any, the designated crisis responder may take such person, or cause by oral or written order such person to be taken into emergency custody in an evaluation and treatment facility for not more than seventy-two hours [.] REV. CODE WASH. § 71.05.153(2)(a) … [A] peace officer may take or cause such person to be taken into custody and immediately delivered to a triage facility, crisis stabilization unit, evaluation and treatment facility, or the emergency department of a local hospital under the following circumstances: (i) Pursuant to subsection (1) … of this section; or (ii) When he or she has reasonable cause to believe that such person [meets the criteria for emergency evaluation].
REV. CODE WASH. § 71.05.230 A person detained for one hundred twenty hours of evaluation and treatment may be committed for not more than fourteen additional days of involuntary intensive treatment or ninety additional days of a less restrictive alternative treatment. A petition may only be filed if the following conditions are met: 1. The professional staff of the facility providing evaluation services has analyzed the person’s condition and finds that the condition is caused by a behavioral health disorder and results in: (a) A likelihood of serious harm; or (b) the person being gravely disabled; and are prepared to testify those conditions are met; and 2. The person has been advised of the need for voluntary treatment and the professional staff of the facility has evidence that he or she has not in good faith volunteered; and 3. The facility providing intensive treatment is certified to provide such treatment by the department or under RCW 71.05.745; and 4. (a)(i) The professional staff of the facility or the designated crisis responder has filed a petition with the court for a fourteen day involuntary detention or a ninety day less restrictive alternative. The petition must be signed by: (A) One physician, physician assistant, or psychiatric advanced registered nurse practitioner; and (B) One physician, physician assistant, psychiatric advanced registered nurse practitioner, or mental health professional. (ii) If the petition is for substance use disorder treatment, the petition may be signed by a substance use disorder professional instead of a mental health professional and by an advanced registered nurse practitioner instead of a psychiatric advanced registered nurse practitioner. The persons signing the petition must have examined the person. (b) If involuntary detention is sought the petition shall state facts that support the finding that such person, as a result of a behavioral health disorder, presents a likelihood of serious harm, or is gravely disabled and that there are no less restrictive alternatives to detention in the best interest of such person or others. The petition shall state specifically that less restrictive alternative treatment was considered and specify why treatment less restrictive than detention is not appropriate. If an involuntary less restrictive alternative is sought, the petition shall state facts that support the finding that such person, as a result of a behavioral health disorder, presents a likelihood of serious harm or is gravely disabled and shall set forth any recommendations for less restrictive alternative treatment services; and 5. A copy of the petition has been served on the detained person, his or her attorney, and his or her guardian, if any, prior to the probable cause hearing; and 6. The court at the time the petition was filed and before the probable cause hearing has appointed counsel to represent such person if no other counsel has appeared; and 7. The petition reflects that the person was informed of the loss of firearm rights if involuntarily committed for mental health treatment; and 8. At the conclusion of the initial commitment period, the professional staff of the agency or facility or the designated crisis responder may petition for an additional period of either 90 days of less restrictive alternative treatment or 90 days of involuntary intensive treatment as provided in RCW 71.05.290; and 9. If the hospital or facility designated to provide less restrictive alternative treatment is other than the facility providing involuntary treatment, the outpatient facility so designated to provide less restrictive alternative treatment has agreed to assume such responsibility. REV. CODE WASH. § 71.05.240. (1) If a petition is filed for up to 14 days of involuntary treatment, 90 days of less restrictive alternative treatment, or 18 months of less restrictive alternative treatment under RCW 71.05.148, the court shall hold a probable cause hearing within 120 hours of the initial detention under RCW 71.05.180, or at a time scheduled under RCW 71.05.148. (2) If the petition is for mental health treatment, the court or the prosecutor at the time of the probable cause hearing and before an order of commitment is entered shall inform the person both orally and in writing that the failure to make a good faith effort to seek voluntary treatment as provided in RCW 71.05.230 will result in the loss of his or her firearm rights if the person is subsequently detained for involuntary treatment under this section. (3) If the person or his or her attorney alleges, prior to the commencement of the hearing, that the person has in good faith volunteered for treatment, the petitioner must show, by preponderance of the evidence, that the person has not in good faith volunteered for appropriate treatment. In order to qualify as a good faith volunteer, the person must abide by procedures and a treatment plan as prescribed by a treatment facility and professional staff. (4) (a) Subject to (b) of this subsection, at the conclusion of the probable cause hearing, if the court finds by a preponderance of the evidence that a person detained for behavioral health treatment, as the result of a behavioral health disorder, presents a likelihood of serious harm, or is gravely disabled, and, after considering less restrictive alternatives to involuntary detention and treatment, finds that no such alternatives are in the best interests of such person or others, the court shall order that such person be detained for involuntary treatment not to exceed 14 days in a facility licensed or certified to provide treatment by the department or under RCW 71.05.745. (b) A court may only order commitment to a secure withdrawal management and stabilization facility or approved substance use disorder treatment program if there is an available facility with adequate space for the person. (c) At the conclusion of the probable cause hearing, if the court finds by a preponderance of the evidence that a person detained for behavioral health treatment, as the result of a behavioral health disorder, presents a likelihood of serious harm or is gravely disabled, but that treatment in a less restrictive setting than detention is in the best interest of such person or others, the court shall order an appropriate less restrictive alternative course of treatment for up to ninety days. (d) If the court finds by a preponderance of the evidence that a person subject to a petition under RCW 71.05.148, as the result of a behavioral health disorder, is in need of assisted outpatient treatment, the court shall order an appropriate less restrictive alternative course of treatment for up to 18 months. (5) An order for less restrictive alternative treatment must name the behavioral health service provider responsible for identifying the services the person will receive in accordance with RCW 71.05.585, and must include a requirement that the person cooperate with the treatment recommendations of the behavioral health service provider. REV. CODE. WASH. § 71.05.280. At the expiration of the fourteen-day period of intensive treatment, a person may be committed for further treatment … if: (1) Such person after having been taken into custody for evaluation and treatment has threatened, attempted, or inflicted: (a) Physical harm upon the person of another or himself or herself, or substantial damage upon the property of others, and (b) as a result of mental disorder presents a likelihood of serious harm; or (2) Such person was taken into custody as a result of conduct in which he or she attempted or inflicted physical harm upon the person of another or himself or herself, or substantial damage upon the property of others, and continues to present, as a result of mental disorder, a likelihood of serious harm; or (3) Such person has been determined to be incompetent and criminal charges have been dismissed …, and has committed acts constituting a felony, and as a result of a mental disorder, presents a substantial likelihood of repeating similar acts… or (4) Such person is gravely disabled. REV. CODE WASH. § 71.05.020(37). "Likelihood of serious harm” means: a) A substantial risk that: (i) Physical harm will be inflicted by a person upon his or her own person, as evidenced by threats or attempts to commit suicide or inflict physical harm on oneself; (ii) physical harm will be inflicted by a person upon another, as evidenced by behavior which has caused harm, substantial pain, or which places another person or persons in reasonable fear of harm to themselves or others; or (iii) physical harm will be inflicted by a person upon the property of others, as evidenced by behavior which has caused substantial loss or damage to the property of others; or b) The person has threatened the physical safety of another and has a history of one or more violent acts. REV. CODE WASH. § 71.05.020(25). “Gravely disabled” means a condition in which a person, as a result of a behavioral health disorder: (a) Is in danger of serious physical harm resulting from a failure to provide for his or her essential human needs of health or safety; or (b) manifests severe deterioration from safe behavior evidenced by repeated and escalating loss of cognitive or volitional control over his or her actions and is not receiving such care as is essential for his or her health or safety; REV. CODE WASH. § 71.05.020(28). “History of one or more violent acts” refers to the period of time ten years prior to the filing of a petition under this chapter, excluding any time spent, but not any violent acts committed, in a behavioral health facility, or in confinement as a result of a criminal conviction; REV. CODE WASH. § 71.05.020(60). “Violent act” means behavior that resulted in homicide, attempted suicide, injury, or substantial loss or damage to property.
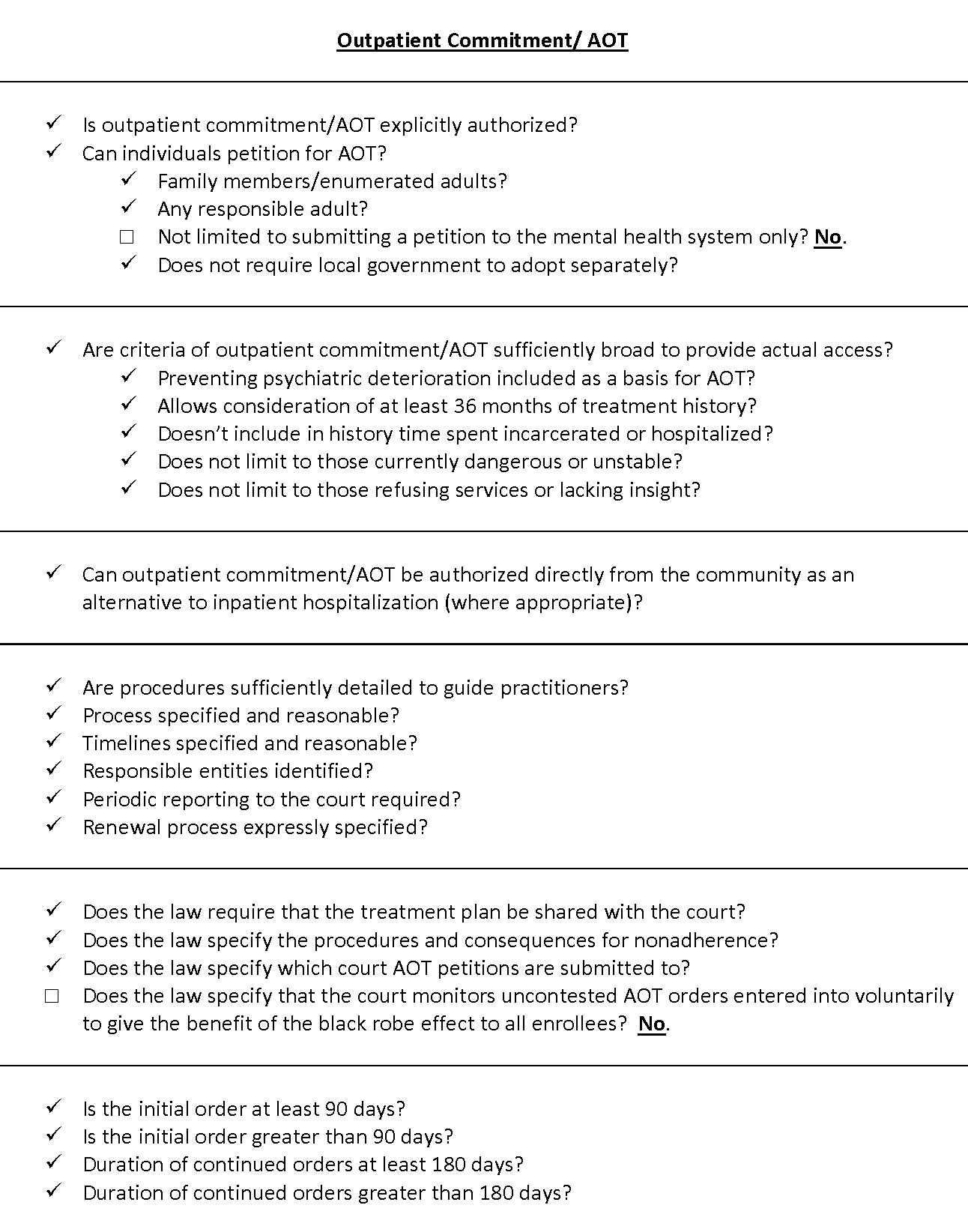
REV. CODE WASH. § 71.05.240(4)(d). If the court finds by a preponderance of the evidence that a person subject to a petition under RCW 71.05.148, as the result of a behavioral health disorder, is in need of assisted outpatient treatment, the court shall order an appropriate less restrictive alternative course of treatment for up to 18 months. REV. CODE WASH. § 71.05.020(30). “In need of assisted outpatient treatment” refers to a person who meets the criteria for assisted outpatient treatment established under RCW 71.05.148; 1. A person is in need of assisted outpatient treatment if the court finds by clear, cogent, and convincing evidence pursuant to a petition filed under this section that: (a) The person has a behavioral health disorder; (b) Based on a clinical determination and in view of the person’s treatment history and current behavior, at least one of the following is true: (i) The person is unlikely to survive safely in the community without supervision and the person’s condition is substantially deteriorating; or (ii) The person is in need of assisted outpatient treatment in order to prevent a relapse or deterioration that would be likely to result in grave disability or a likelihood of serious harm to the person or to others; (c) The person has a history of lack of compliance with treatment for his or her behavioral health disorder that has: (i) At least twice within the 36 months prior to the filing of the petition been a significant factor in necessitating hospitalization of the person, or the person’s receipt of services in a forensic or other mental health unit of a state correctional facility or local correctional facility, provided that the 36-month period shall be extended by the length of any hospitalization or incarceration of the person that occurred within the 36-month period; (ii) At least twice within the 36 months prior to the filing of the petition been a significant factor in necessitating emergency medical care or hospitalization for behavioral health-related medical conditions including overdose, infected abscesses, sepsis, endocarditis, or other maladies, or a significant factor in behavior which resulted in the person’s incarceration in a state or local correctional facility; or (iii) Resulted in one or more violent acts, threats, or attempts to cause serious physical harm to the person or another within the 48 months prior to the filing of the petition, provided that the 48-month period shall be extended by the length of any hospitalization or incarceration of the person that occurred during the 48-month period; (d) Participation in an assisted outpatient treatment program would be the least restrictive alternative necessary to ensure the person’s recovery and stability; and (e) The person will benefit from assisted outpatient treatment.
Recommended updates to treatment laws
- 1
Amend Wash. Rev. Code §§ 71.05.150(1) and 71.05.153(1) to authorize citizen right of petition for at least enumerated citizens, preferably any responsible adult, for emergency evaluation
- 2
Amend Wash. Rev. Code § 71.05.230(4)(a) to authorize citizen right of petition for at least enumerated citizens, preferably any responsible adult, for inpatient commitment
- 3
Amend Wash. Rev. Code § 71.05.203 to authorize citizen right of petition directly to court (currently allows petition only to department of health) for at least enumerated citizens, preferably any responsible adult, for outpatient commitment
- 4
Adopt express procedures for the court to monitor uncontested AOT orders entered into voluntarily to give the benefit of the black robe effect to all enrollees